LOWER EYELID SURGERY
REJUVENATE YOUR LOOK
WITH LOWER BLEPHAROPLASTY
UNDERSTANDING UPPER EYELID AGING AND BLEPHAROPLASTY
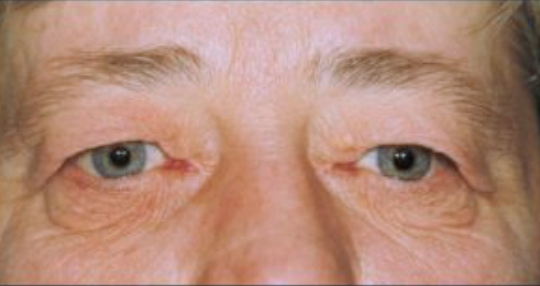
48 year old female pre-op.

3 months post lower and upper blepharoplasty

42 year old pre-op
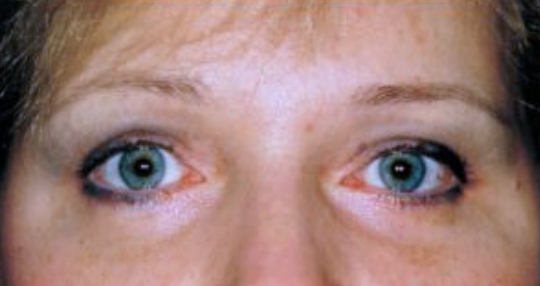
3 months post lower and upper blepharoplasty
As one ages, the lower lid tissues begin to relax and stretch. The skin becomes thinner, wrinkled and redundant. Sun exposure, allergies or recurrent swelling may accelerate these nonspecific changes. In some individuals, this process may be hereditary. The result is an excess of eyelid skin referred to as “dermatochalasis”. Stretching and relaxation of the eyelid tissues (orbital septum) will also allow migration of the orbital fat into the eyelids (fat prolapse). As a result, a “fullness” of the lower eyelids develops, which may worsen over time. The excess lid skin and fat bags create a tired look, may cause the patient to look older than they are. Having eyelid surgery to remove the excess skin and fat is referred to as “Blepharoplasty”. Removal of the excess skin and fat can restore a younger; more rested appearance.
Assessing eyebrow position is crucial for upper eyelid surgery candidates, as eyebrows also droop with age, exacerbating the appearance of sagging eyelids. Some patients may need both brow elevation and blepharoplasty for optimal cosmetic and functional results.
ABOUT LOWER BLEPHAROPLASTY II SURGERY
Blepharoplasty surgery will remove the bulges and shadows created by fat herniation as well as the excess skin that is becoming redundant and hanging downwards (Figure 1 and 2). Many patients want “all” the lines removed on their lid. With lower blepharoplasty, the lines will diminish in their appearance but to remove them all, may pull the eyelid downward and prevent normal eyelid closure. If the eyelids get pulled down a “roundeyed” appearance is created. If the eyes don’t close properly, dry irritable eyes develop. Laser skin resurfacing is more effective in removing the fine lines than scalpel but even with laser it may not be possible to remove all of them.
The goals of surgery therefore, are to remove enough tissue to restore a younger, healthier, more rested appearance, yet leave enough lid tissue on the eyelid to allow proper eyelid opening and closing, and without any distortion or change in the natural almond-shaped eyelid contour.
A preoperative eye check is important to assess the visual acuity, tear film, strength of lid closure, symmetry of eyelid openings, and status of any other eye problems. The pre-existence of dry eyes, facial nerve palsy, eyelid laxity, punctual malposition, prominent eyeballs, etc., will have a bearing on the amount of tissue removed during the lid surgery and whether the lower eyelid requires a tightening procedure at the same time.
Lower blepharoplasty surgery is an out-patient procedure performed either in the office, or hospital, under local anesthesia with oral sedation and/or intravenous sedation. During scalpel surgery, incisions are made just below the eyelashes. The eyelashes are left alone and well preserved. Skin is dissected away from the underlying muscle which is then is dissected away from underlying fatty tissue. If a lot of fat is present a small amount is removed. In some patients the fat is actually mobilized into a sunken area along the orbital rim to hide shadows on the lower eyelid (“fat transfer procedure”).Bleeding vessels are gently cauterized with a cautery machine. The muscle tissue is re-suspended to the lateral orbital rim. The skin is re-draped and trimmed. The skin edges are then approximated and sutured together with absorbable sutures. The incision blends into the lid very nicely and with normal tissue healing and a little make-up is hard to see by 2 weeks. The incision gradually matures, settles and becomes barely noticeable over the next 1 to 3 months.
If only fatty tissue needs to be removed from the lower lids (no skin removal), the surgery can be preformed from inside the eyelid. This is known as a “transconjuntival blepharoplasty”and is a very quick procedure with rapid recovery.
Following surgery, rest with cool compresses (frozen peas, ice, gel packs, etc.) over the eyelids 4 to 6 times daily for 30-60 minutes is required for about 3 days. Patients are able to get up and walk around but are cautioned to avoid heavy lifting, straining and excess activity to prevent any stress on the eyelid incision and potential bleeding. Discomfort is usually minimal and relieved with acetaminophen (Tylenol). Most individuals will have swelling and some degree of bruising in the first week. It is best to be off work and away from social events for about 1 week. Makeup can be applied after one week. Complete tissue healing usually occurs by 2 to 3 months.
The eyelid blink rate may temporarily slow down post surgery and, as a result, the eyes may have a gritty or sandy feeling. Artificial tears during the day and lubricating ointment at night are commonly used to keep the eyes moist during the healing process. Blurry vision may occur during the healing period as a result of the decrease in eyelid blink rate or ointment getting into the eye but returns to normal over the next few weeks. Infection, excessive pain, and bleeding with hematoma formation are very uncommon. If infection develops, antibiotics may be required either orally or intravenously. Pain should be minimal if any. If pain is present and severe, it is important to notify the physician who did the surgery, or the physician “on-call” for further assessment. Bleeding into the eyelid tissue with hematoma formation is very uncommon. Most hematomas settle on their own. If they are large and prevent the eyelid from opening, drainage is sometimes required. Loss of vision has been reported following lower blepharoplsty surgery but fortunately is extremely rare and very few blepharoplasty surgeons will ever encounter it. The exact incidence is unknown but is probably in the order of 1 in 2,500, i.e. .04%. The cause is usually orbital bleeding with a build up of blood behind the eye (retrobulbar hemorrhage).
Once the healing process has settled (average 2 to 3 months), if there is any lid asymmetry, a touchup procedure may be required in less than 5% of patients.
The potential complications associated with lower blepharoplasty surgery are eye related. It is important to have the surgery done by someone who has a thorough knowledge of the eye and is able to manage the potential eye problems that occaisionally occur.
In over 99% of cases the answer is no. If however, the lower lid fat bags are so large they actually sit on the bifocal part of the patients glasses and cause a restriction of the reading vision, Ohip may cover the surgery. This situation however, occurs rarely and photographs are required to show the problem. They do not cover lower eyelid surgery for any other reason.

LOOK YOUNGER, FEEL REFRESHED
Contact us today to discover how we can help you achieve a more youthful, refreshed look.



