



Volume 7 • Issue 1
Ptosis In Adults

by David R. Jordan
M.D., F.A.C.S., F.R.C.S.(C)
INTRODUCTION
Ptosis (pronounced “toe-sis”) refers to a drooping of the upper eyelid and may affect one or both eyelids. If the ptosis develops with age it is referred to as acquired ptosis. When the eyes are in straight ahead gaze, the upper lids should rest approximately 2 mm below the superior limbus. With ptosis, the lid(s) may droop only slightly (0.5–1 mm) or may droop enough to partially or completely cover the pupil (3–4 mm) which subsequently restricts or obscures vision. [Figure 1a]
What Are The Causes Of Acquired Ptosis?
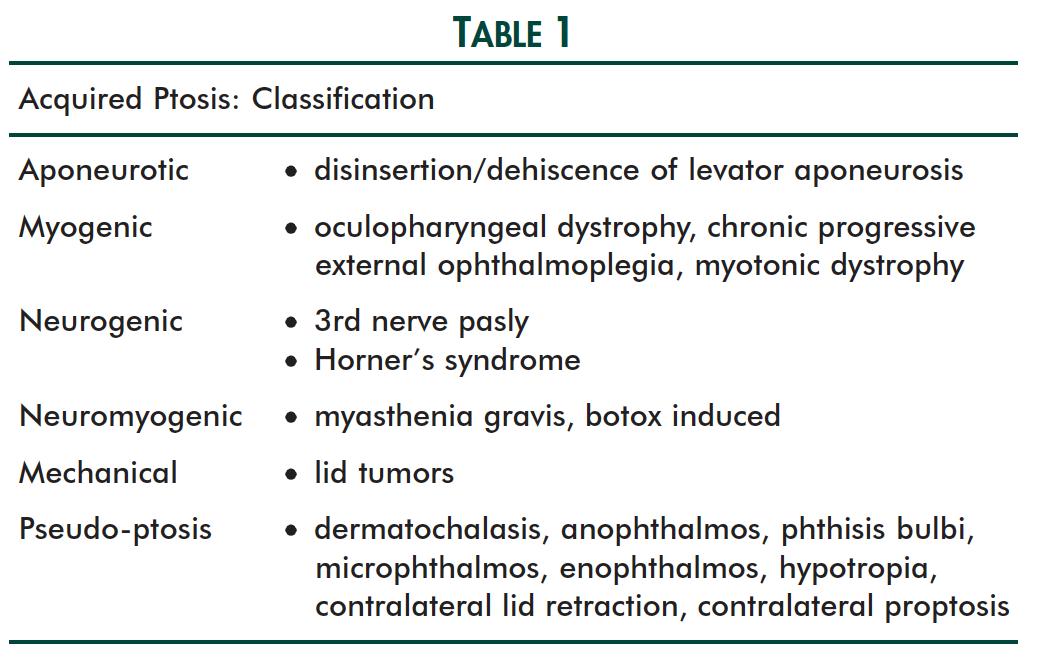
Acquired ptosis may be divided into Aponeurotic, Myogenic, Neurogenic, Neuromyogenic and/or Mechanical causes [Table 1].
Aponeurotic Ptosis
Aponeurotic ptosis is the most common variety of adult acquired ptosis and is a result of the aging process in most cases. [Figure 1a/1b] The levator aponeurosis (which attaches the levator muscle to the tarsal plate) becomes thin with age and may become unattached to the tarsal plate (dehiscence or disinsertion). As a result the lid falls. On examination, the upper eyelid crease is characteristically high and there is excellent levator function on examination. The upper lid tissues occasionally are so thin that the iris may be visualized through the lid. Other causes of an aponeurotic disinsertion type ptosis include trauma to the eyelid, recurrent edema of the upper lids, previous ocular surgery, or pulling on the lids during contact lens insertion.

Figure 1a –
Bilateral acquired ptosis.

Figure 1b –
Post levator advancement surgery.
Myogenic Ptosis
In myogenic ptosis, the problem is in the levator muscle itself. A degenerative process occurs in the muscle fibers. As a result the muscle weakens and the lid falls. Examples include Myotonic Dystrophy, Oculopharyngeal Dystrophy and Chronic Progressive External Ophthalmoplegia. Oculopharyngeal Dystrophy is common in French Canadian families and is passed down through the generations as an autosomal dominant trait. The patients characteristically develop drooping of the upper lids in their late 40’s and 50’s and have difficulty swallowing their food. [Figure 2a/2b] Some of the individuals will develop muscular weakness in other parts of their body while others will remain with the droopy lids and difficulty swallowing. The difficulty swallowing can be severe and may lead to death from choking.

Figure 2a – Bilateral oculophorynged dystrophy ptosis.

Figure 2b – Post-operative appearance.
Neurogenic Ptosis
Neurogenic ptosis is a result of a nerve injury, either the third nerve or the sympathetic nerves to the upper lid. A third nerve palsy may result from trauma, diabetes, aneurysm or idiopathic. Classic-ally, one lid is completely ptotic. When you lift the lid the eye itself is shifted downward and outwards as a result of the unopposed action of the 4th and sixth cranial nerve. [Figure 3] The pupil is also dilated.

Figure 3 – 3rd nerve palsy with ptosis on patients left upper lid. Left eye is pointed down and outward.
Horner’s syndrome is a result of injury to the sympathetic nerve supply to the upper eyelid. Classically, there is a minor degree of ptosis, miosis, anhidrosis on one-half of the face and apparent enophthalmos as a result of lid fissure narrowing.
Neuromyogenic Ptosis
The classic type of ptosis in this category is Myasthenia Gravis. Our present under-standing of myasthenia is that it is an acquired immune complex disease occurring at the neuromuscular junction with blocking and degradation of acetyl-choline receptors. The neurotransmitter acetylcholine is released from the nerve terminals but cannot effectively stimulate the muscle as the acetylcholine receptors are blocked. Muscle function is therefore weakened. Myasthenia Gravis is a chronic disease characterized by fluctuating weakness of voluntary muscles. Weakness increases during prolonged activity while strength is restored following rest. There is also dramatic improvement following intravenous administration of anticholinesterases which temporarily allow an increase in acetylcholine at the neuro-muscular junction. [Figure 4a/4b] Myasthenia Gravis not uncommonly presents with ptosis as the initial manifestation. Some individuals develop generalized myasthenia while others will remain with only ocular involvement. The hallmarks of this condition is “variable lid height”. The lid may be of normal height in the morning but gradually droops as the day goes on. If the process generalizes, the muscles of facial expression, mastication, swallowing, and speech are next most frequently affected. The flexors and extensors of the neck shoulder girdle and hips are less often involved. The course of the disease is variable, remissions can occur without explanation.

Figure 4a – Ptosis of patients left upper lid.

Figure 4b – Resolution of ptosis following tensilon.
Mechanical Ptosis
An upper lid tumor may act as a weight and as a result cause the lid to droop. Usually the cause is obvious as the lid tumor should be quite visible. [Figure 5]

Figure 5 – A Chalazion causing ptosis.
Pseudo-ptosis
Pseudo-ptosis refers to those conditions that mimic true ptosis. Dermatochalasis is a type of pseudo-ptosis characterized by excess skin hanging over the upper eyelid margin. It gives the appearance of a droopy lid but the problem is skin excess rather than a levator aponeurosis or muscle problem. Blepharoplasty is generally required. In microphthalmos, anophthalmos, enophthalmos and phthisis bulbi there is a loss of volume in the eye or orbit, causing the vertical dimensions of the palpebral fissure to narrow and thus mimic a true ptosis. In hypotropic eyes, the upper eyelid follows the globe inferiorly, simulating a true ptosis. Here, when the eye is covered and the hypotropic eye picks up fixation, the pseudo-ptosis disappears. Other causes of pseudo-ptosis include contralateral lid retraction and contralateral proptosis.
What are the Signs and Symptoms of Adult Acquired Ptosis?
The most obvious sign is a droopy upper lid. This gives the adult a sleepy look. The patient may complain of peripheral visual field loss or fatigue from attempting to elevate the droopy lid. Reading may be difficult as the ptotic eyelid tends to block the visual axis when the eye is looking down. Adults with bilateral ptosis will often tip their heads back to see past their eyelids or raise their eyebrows in an effort to raise their lids. If the ptosis is severe they may bump into things at a forehead level (cupboard doors).
When is Treatment Required?
Treatment is required when the patient becomes symptomatic. Surprisingly, in some patients, the process has occurred so slowly they have adjusted to the lower lid level without being aware of it causing a problem. Generally,when the lids have dropped low enough to cause a visual field loss, the patient is having trouble when reading, or the patient is bumping his/her forehead on things, lid elevation should be considered.
How is Adult Ptosis Treated?
Treatment when necessary, is surgical in the majority of acquired ptosis patients and is done as an outpatient under local anesthesia. It is important to do the surgery under local anesthesia as this gives the surgeon a better idea of how much to raise the eyelids. The patient has either oral or intravenous sedation as well as a local anaesthesia in the eyelid. A small incision is made in the eyelid crease line and the thinned levator aponeurosis is isolated and filled from surrounding tissues. The levator aponeurosis is advanced onto the tarsal plate and temporarily tied there. The patient is sat up and if the lid height is not just right, the patient can be laid down and have the suture adjusted. Once the right height is achieved the lid skin is closed. Postoperatively there is usually some mild lid swelling which settles over the first 2 weeks or so. Ice packs in the first 3 days are very helpful to keep the swelling at a minimum. The patient should be off work for 4–7 days. Post-operatively patients are generally quite relieved to have the visual obstruction removed.
Myasthenia Gravis is one example of an acquired ptosis that doesn’t require surgery. In this situation, treatment involves medication (anticholinesterases) which lead to an increase level of neurotransmitters (acetylcholine) at the nerve-muscle junction. The additional acetylcholine leads to an improvement in ptosis.
For some ptosis with extremely poor function (ex. oculopharyngeal dystrophy, myotonic dystrophy, chronic progressive external ophthalmoplegia) there is not enough levator or muscle function to adjust the lid height. In these instances an alternative surgery may be suggested, termed a “Frontalis Sling”. In this situation, a flexible silicone rod, fascia lata, or strip of gortex, is passed from the frontalis muscle, under the eyebrow to the eyelid. As the patient lifts the brow, the eyelid will be raised as a result of the silicone rod tension within the upper eyelid.
What About The Brows, Lid Skin And Fat?
Aging patients with drooping eyelids may also have excess lid skin (dermatochalasis) and fat prolapse and/or a low brow height, both of which can cause a drooping eyelid appearance. Surgery for these latter two problems may be required and can be performed at the same time as levator advancement surgery but are no longer covered by insurance (OHIP).
What are the Risks of ptosis surgery?
Bleeding and infection are possible but extremely rare. Patients on Aspirin and antiarthritic medication, Vitamin E or Ginko Biloba are asked to stop these for a few days prior to and post surgery, to reduce the chance of bleeding and bruising. Under or over correction of the lid height can occasionally occur. If the lid height anomaly is obvious, a suture adjustment may be required in the first to two weeks. A temporary inability to fully close the eye after ptosis surgery is common and generally resolves in most over a few weeks. The eyelids do not remain “stuck open”. During this time period when the lids are not fully closing it is important to use lubricating drops and ointment to keep the cornea moist.
Summary
Ptosis in adults is common and most often due to a weakening of the levator aponeurosis which is responsible for keeping the lid open. The droopy lid(s) can be successfully treated with little risk and minimal down time as an outpatient under local anaesthesia.
If you have any questions regarding the topics of this newsletter, or requests for future topics of InSight, please contact Dr. David R. Jordan office by telephone at (613) 563-3800.

